Annotation
In this retrospective case series, chest CT scans of 21 patients from China with clinical manifestations infected with the new 2019 coronavirus (2019-nCoV) were analyzed; emphasis was placed on identifying and characterizing the most common features. Typical CT signs included bilateral “frosted glass” thickening of the pulmonary parenchyma and consolidation zones, which sometimes had a rounded shape and extended to the peripheral parts of the lungs. Notably, pulmonary cavitations, solitary nodules, pleural effusion and lymphadenopathy were absent. At further CT control in this group of patients during the study period, mild or moderate progression of changes was often revealed, which was manifested in the increase in the degree and density of areas of lung tissue thickening.Brief overview
Infection caused by the new 2019 coronavirus shows characteristic signs on chest CT scans that aid the radiologist in early detection and diagnosis of this new global public health emergency.Key findings
- Of the 21 patients with 2019-nCoV infection, 15 (71%) had lesions in more than two lobes on chest CT, 12 (57%) visualized frosted glass-like consolidations, seven (33%) had rounded consolidations, seven (33%) had peripheral spread, six (29%) had foci of both consolidation and frosted glass-like consolidations, and four (19%) had a crazy-paving pattern.
- Pulmonary cavitations, solitary pulmonary nodules, pleural effusion and lymphadenopathy were absent.
- Fourteen percent of patients (three of 21) had no pathologic changes on CT scan.
Introduction
On 31 December 2019, the World Health Organization (WHO) was notified of several cases of a respiratory disease of unknown origin detected in Wuhan City, Hubei Province, China, with clinical manifestations resembling viral pneumonia symptoms and presenting with fever, cough, and shortness of breath. As of January 30, 2020, WHO has designated the outbreak as a global health emergency. Chest X-rays often showed pulmonary darkening in patients. By January 3, 2020, 44 patients with this illness of unclear etiology had been reported to WHO, with preliminary epidemiological investigation indicating that most patients worked or were frequent visitors to the Huangan seafood wholesale market [1]. Analysis of bronchoalveolar lavage fluid samples and electron microscopy showed that the causative agent was coronavirus, with its characteristic ultrastructural morphology in electron microscopy, which is due to the presence of spike-like outgrowths emanating from the viral envelope, resembling the appearance of a corona. The discovered virus has been provisionally named the new 2019 coronavirus (2019-nCoV). Coronaviruses belong to the family Coronaviridae, a genus Nidovarales and family that includes viruses that cause diseases ranging from the common cold to severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) [2]. The SARS outbreak began in southern China and was recognized as a global public health threat in March 2003, and from November 2002 to July 2003 resulted in 774 deaths out of 8098 infected individuals [3]. MERS was first reported in 2012 in Saudi Arabia, and to date there have been 858 deaths per 2494 infections [4]. As of January 28, 2020, there are 4,593 confirmed cases worldwide. Of these, 4,537 are in China and 56 from 14 other countries. In addition, there are another 6,973 suspected cases in China. As of January 28, 2020, there have been 106 fatal cases – all in China [5]. On January 30, 2020, WHO declared Chinese coronavirus a global health emergency. An initial prospective analysis of clinical data from 41 initially admitted patients with laboratory-confirmed 2019-nCoV in Wuhan showed that 2019-nCoV caused severe illness clinically similar to SARS, sometimes resulting in the need for ICU hospitalization (13 of 41 [32%]) and death (6 of 41 [15%]). All patients with pneumonia in this study had changes on chest computed tomography: preliminary reports showed bilateral thickening of the lung parenchyma in all patients [6]. In this article, we describe and characterize the key CT features found in a cohort of 21 patients infected with 2019-nCoV in China to familiarize radiologists and other clinical team members with the radiologic manifestations of this emerging disease. Early recognition of the disease can expedite treatment and provide early patient isolation, it will also enable early surveillance, containment and public health response to this infectious disease.Materials and methods
Patients and chest CT
Our institutional review board waived the requirement to obtain written informed consent for retrospective analyses of this case series, in which depersonalized data were evaluated and no potential risk to patients was anticipated. To prevent potential breaches of confidentiality, patient-researcher communication was not available. Between January 18, 2020 and January 27, 2020, 21 patients with confirmed 2019-nCoV infection were admitted to three hospitals in three provinces in China; all underwent chest CT scans. Ten patients from Zhuhai (Guangdong Province) underwent CT scans with 1-mm-thick slices using a CT CT scanner UCT 760 (United Imaging, Shanghai, China). Nine patients were from Nanchang (Jiangxi Province) Tomography with 8-mm-thick slices using an Emotion 16 scanner (Siemens Healthineers). Two patients were from Qingdao (Shandong Province) and underwent a study with a slice thickness of 5 mm, one using a BrightSpeed scanner (GE Medical Systems) and one using an Aquilion ONE scanner (Toshiba Medical Systems). All studies were performed in the patient’s supine position at inspiratory height, without contrast agent administration. All patients had confirmed 2019-nCov infection by laboratory testing of bronchoalveolar lavage fluid, endotracheal aspirate, nasopharyngeal swab, or oropharyngeal swab. Patient selection for this study was continuous at each of the three institutions, and no exclusion criteria were applied (Table 1). In addition to information on age and sex, the clinical information collected included data on the severity and course of symptoms, and epidemiologic history, including information on patient travel. Table 1 | General patient data (n = 21)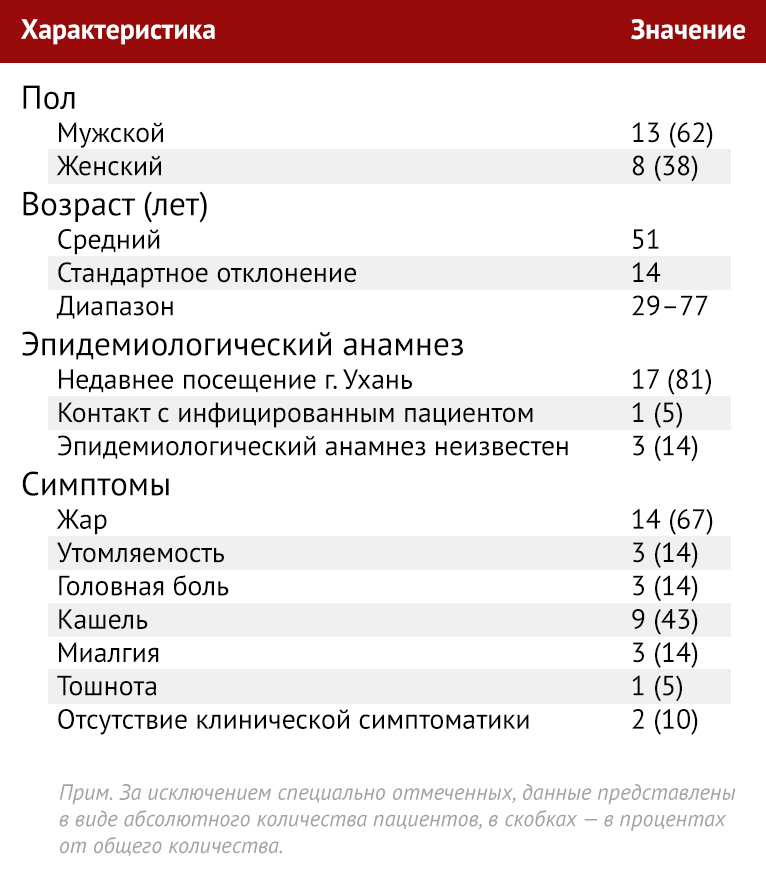
Analysis of CT studies
Each CT study was reviewed by two radiologists trained in cardiothoracic radiology with approximately 5 years of experience each (M.C. and A.B.) using a viewing console. Studies were reviewed independently and final results were formed by consensus. If there was disagreement between the two main interpretations, a third qualified cardiothoracic radiologist with 10 years of experience made the final judgment. Negative control and blinded method were not used. For each of the 21 patients, the initial (conducted on admission–note.) CT examinations were evaluated for the following characteristics: (a) the presence of frosted-glass type seals, (b) the presence of consolidation, (c) the number of lobes to which frosted-glass type seals and consolidation areas extended, (d) the extent of lobe involvement in addition to a general “lung lesion severity scale”, (d) presence of nodules, (e) presence of pleural effusion, (j) presence of thoracic lymphadenopathy (defined as lymph node size ≥10 mm in the short axis dimension), and (z) presence of underlying lower respiratory disease such as emphysema or fibrosis. Other CT symptoms, such as cavitations, reticulation, thickening of the interval septa, calcifications, and bronchiectasis, were also noted. Frosted-glass consolidation was defined as an increase in lung tissue density in the form of haze with preserved visualization of bronchial and vascular margins, and consolidation was defined as an increase in lung tissue density with darkening of vascular margins and airway walls [7]. Each of the five lung lobes was graded according to the degree of involvement and categorized as absent (0%), minimal (1-25%), mild (26-50%), moderate (51-75%), or severe (76- 100%). Absence of involvement corresponded to 0 points, minimal involvement corresponded to 1 point, mild involvement corresponded to 2 points, moderate involvement corresponded to 3 points, and severe involvement corresponded to 4 points. The result of the overall “lung lesion severity scale” was generated by summing the scores from each of the five lung lobes (range of possible scores 0-20). Eight patients underwent a control chest CT scan during the study. These scans were also evaluated to determine change or progression over time, which was qualitatively assessed using a consensus approach by two radiologists (M.C. and A.B.).Results
Thirteen men and 8 women in the age range 29-77 years participated in the study; mean age ± standard deviation, 51 years ±14.Frosted glass seals and consolidation
Of the 21 initial CT studies, three (14%) patients did not have frosted-glass consolidations; in essence, these three patients had no CT signs of chest pathology on admission (Table 2). Of the 18 patients in whom areas of “frosted glass” type consolidation or consolidation were visualized, only “frosted glass” type consolidations were noted in 12 (no consolidation). No patient had areas of consolidation of lung tissue without “frosted glass” consolidation. Table 2 | CT signs found in 21 patients on initial examination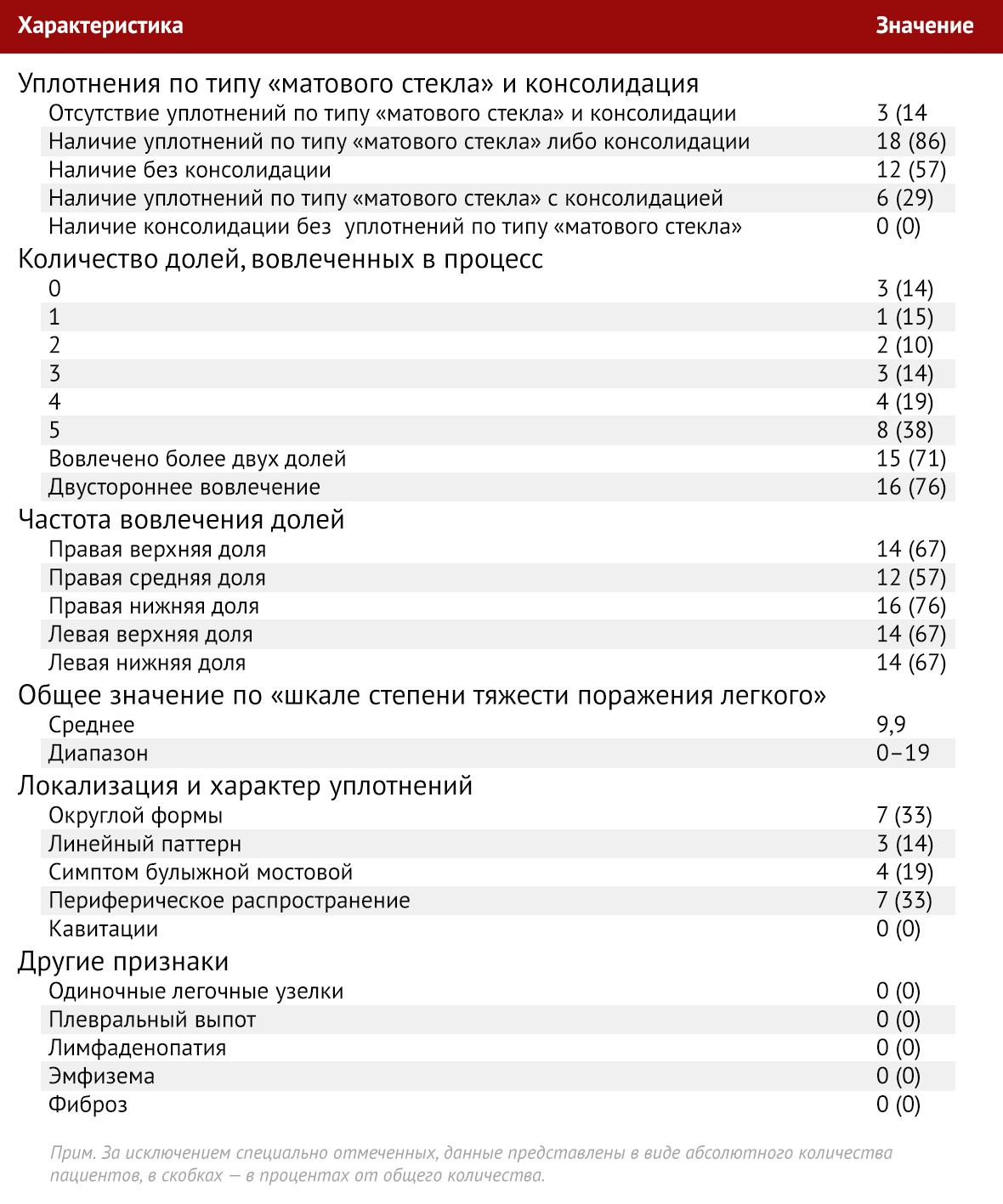
Prevalence and patterns of increased lung tissue density
With the exception of three patients with a normal initial chest CT scan, the remaining 18 of 21 patients (86%) had changes affecting at least one lobe by definition. Of the 21 patients, one patient (5%) had one lobe affected, two patients (10%) had changes defined in two lobes, three patients (14%) had three lobes affected, four patients (19%) had four lobes affected, and eight patients (38%) had pathologic changes extending to all five lobes. The right upper lobe was involved in 14 of 21 patients on initial CT examination (67%), the right middle lobe in 12 (57%), the right lower lobe in 16 (76%), and changes in the left upper lobe were noted in 14 (67%) patients and the left lower lobe in 14 (67%). Of the 18 patients with increased lung density, 16 had bilateral changes and two had unilateral changes (both had right lung lesions). The total score on the “lung lesion severity scale” ranged from 0 (with three normal CT studies) to a maximum of 19 with a mean score of 9.9. The patient with the highest severity score was admitted to the ICU (Figure 1).
Figure 1. A 29-year-old male with unknown epidemiologic history, admitted with complaints of fever, cough and was immediately referred to the ICU. (a) Axial thin-slice CT scan without contrast agent injection demonstrates diffuse areas of frosted glass-like consolidation of a draining nature on both sides (white arrows) and areas of consolidation (black arrows). (b) Axial CT scan without contrast injection shows that changes in the right middle and lower lobes tend to be peripherally localized (arrows).

Figure 2. A 36-year-old male with after a recent trip to Wuhan, complained of fever, fatigue and myalgia. Coronal thin-slice CT scan without contrast agent injection shows areas of “frosted glass”-type rounded thickening in both upper lobes (arrows).

Figure 3: A 66-year-old woman with fever and productive cough after a recent trip to Wuhan. Axial thin-slice collimated CT scan without contrast agent injection demonstrates the “cobblestone symptom”: a reticular pattern of thickening of the interlobular septa and linear thickened interstitium with a frosted glass-like lesion in the right lower lobe (arrow).

Figure 4. A 69-year-old man, a recent visitor to Wuhan, admitted with fever. Axial thin-slice CT scan without contrast agent injection shows areas of “frosted glass” type thickening in the lower lobes with a marked tendency to peripheral spread (arrows).
CT control data in dynamics
During the study period, eight patients underwent repeat chest CT scans, and one patient underwent two control CT scans (Table 3). The mean time between the initial chest CT and the follow-up CT was 2.5 days (range 1-4 days). In one of eight patients (13%), the initial and follow-up chest CTs showed no pathologic features, with no change in follow-up. None of the patients had positive CT dynamics. Five of eight patients (63 %) had slight progression of changes, and two (25 %) had moderate progression. No patient demonstrated significant negative dynamics. One patient with a slight worsening of the CT pattern over time, as determined by the first follow-up CT scan performed 1 day after the initial examination, underwent a second follow-up CT scan 3 days later (4 days after the initial CT examination). On repeat CT follow-up, there was a marked progression of changes in the form of an increase in the number of areas of consolidation and consolidation density. Finally, in one patient who had no changes on the initial chest CT scan, a new single, single, rounded, frosted-glass-type consolidation in the periphery was found on control CT 3 days later (Figure 5). Table 3 | Qualitative assessment of changes on follow-up CT scanning over time in eight patients

Figure 5. A 43-year-old woman, a recent visitor to Wuhan, admitted with fever. (a) Axial thin-slice CT scan without contrast agent injection from January 18, 2020 CT image shows no pathologic changes on the lung side. (b) A control CT image obtained on January 21, 2020, shows a new solitary rounded peripheral focal frosted glass-like mass in the right lower lobe (arrow).